


Here's how a physician-led model changes the math, and the outcomes.
Across employer benefit programs and health plans alike, MSK spend is high and outcomes are lacking. The culprit isn’t access. It’s the order in which decisions get made.
Musculoskeletal conditions, back pain, knee pain, shoulder injuries, joint problems, are among the most common reasons employees miss work, seek care, and drive up healthcare spend. And yet, in most benefits programs, MSK is also one of the most poorly managed categories in the entire plan.
The reason isn't a lack of access to care, or even under-utilization. It's that patients are routinely routed into the wrong kind of care, at the wrong time, without the clinical judgment needed to stop a very predictable, and very expensive, cascade.
At Vori Health, we call this the MSK cascade. And we built our model specifically to interrupt it.
Why MSK Is a Decision Problem
Across the U.S. healthcare system, MSK conditions are frequently mismanaged, not because patients aren't receiving care, but because the decision about what kind of care they need is made by the wrong person, too late, or not made at all.
Consider how a typical MSK episode unfolds for your employees today:
- An employee develops back pain or a knee problem and goes to their primary care physician (PCP).
- The PCP, who receives only about 200 hours of MSK training across a three-year residency, orders an MRI, even though clinical guidelines don't support it at this stage.
- The MRI returns findings. In asymptomatic adults, MRI findings are almost universal: 96% of shoulders over age 40, 89–97% of knees, and 68% of lumbar spines show abnormalities on imaging, regardless of whether those findings are causing the patient's symptoms.
- A finding triggers a surgical referral. Early MRI is associated with a 13x higher probability of lumbar surgery, even in patients who have no red flags and no clinical indication for an operation.
- Surgery proceeds. And in 38% of lumbar spine cases and 34% of total knee replacement cases, it proceeds without appropriate clinical indications.
MSK costs don't spiral because of one bad decision. They spiral because nobody stopped the first one.
The financial consequences are significant. Guideline-discordant MSK care, the kind that results from this cascade, increases annual healthcare costs by an average of $4,000 per patient. And the clinical consequences are just as serious: more than 41% of lumbar spinal fusion patients fail to achieve meaningful improvement in pain or function at one year, and nearly 1 in 5 require reoperation within four years.
This is the problem Vori was designed to solve.
Why Physician-Led MSK Care Is Different
Most MSK solutions on the market today are built around physical therapy as the primary, and often only, clinical touchpoint. Direct-access PT models have their place, and for many patients, PT is exactly the right first step. But PT alone has a fundamental limitation: physical therapists are trained in the musculoskeletal system, not the whole patient.
Where PT-only models have limits
Non-musculoskeletal causes of MSK symptoms occur in 2–22% of patients. For older adults, the risk is even higher.
A patient presenting with shoulder pain may have a cardiac referral pattern.
A patient with back pain may have an early spinal malignancy.
These are not hypothetical edge cases, missed serious pathology, including fractures, neoplasms, and cauda equina syndrome, occurs in approximately 2.3% of MSK patient episodes.
Additionally, approximately 35–40% of MSK patients do not achieve clinically meaningful improvement with physical therapy alone. When PT doesn't work, patients are escalated, often back to a PCP or directly to a surgeon, and the cascade continues.
What physician-led care adds
Vori's model is built around a specialty MSK physician as the clinical anchor, not necessarily the first person a patient sees, but always present in the care team, guiding triage and oversight from day one.
When a patient enters the Vori system, they are triaged through a clinically-guided, tech-enabled process that determines the right level of care for their specific condition:
- PT only
- Physician evaluation + PT
- Physician evaluation with imaging when clinically warranted
The physician doesn't insert themselves into every case, that would be unnecessary and inefficient. What they do is ensure that no patient is sent down a pathway that isn't supported by the clinical evidence. That's the difference between an MSK program and an MSK medical practice.
A specialty MSK physician is always part of the integrated care team, available when needed, not inserted when unnecessary. The goal is not more physician contact. It is better decisions at every step.
What Happens Without Physician-Led Oversight
The data on non-physician-led MSK pathways is consistent: without clinical triage by a physician, costs rise, outcomes suffer, and the cascade is difficult to stop once it begins.
The imaging problem
In standard healthcare settings, 12–18.5% of patients with low back pain receive a lumbar MRI, and 26–44% of those orders don't meet appropriate use criteria. Inappropriate imaging is not a minor inefficiency. It is the trigger that starts the cascade.
Once an MRI is ordered, incidental findings are nearly guaranteed. And once a finding appears in the record, the clinical and psychological pull toward intervention becomes very difficult to resist, even when the finding is unrelated to the patient's symptoms. Research shows that when orthopedic groups acquire MRI equipment and begin self-referring, the probability of a patient undergoing surgery increases by 34 percentage points.
The surgery problem
Inappropriate MSK surgery is common across every major procedure category: 34–35% of knee arthroscopies for degenerative disease, 34% of total knee replacements, and 38% of lumbar spine surgeries are performed without appropriate clinical indications.
For your plan, this means your employees are undergoing operations they may not need, and living with the consequences. More than 41% of spinal fusion patients fail to achieve meaningful improvement. Nearly 1 in 5 need a second surgery. And spinal fusions cost $60,000–$110,000 per procedure, with the U.S. spending over $16 billion annually on them.
The chronic pain problem
Perhaps most importantly, delayed or misdirected MSK care significantly increases the risk that an acute condition becomes chronic. Patients who receive early, appropriate intervention have an 8-fold lower risk of developing chronic pain compared to those who receive usual care. The longer the cascade runs before it's interrupted, the harder it is to stop.
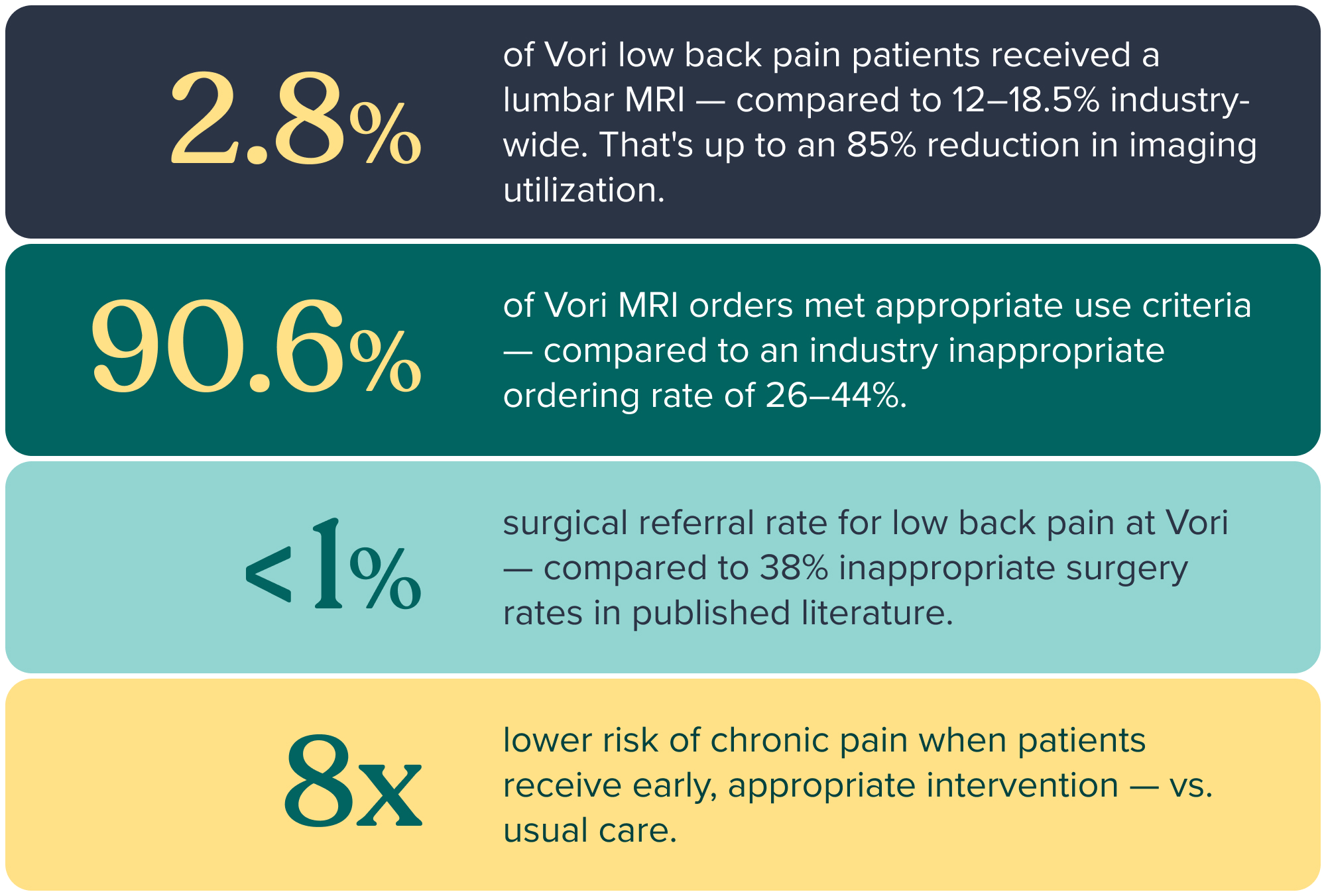
The Vori Difference in Numbers
Vori's physician-led model produces measurable results, documented in our patient outcomes data and validated against published literature.
What This Means for Your Benefits Program
If your current MSK benefits are built around direct-access PT, a telehealth-only model, or no structured MSK management at all, your employees are likely moving through the cascade right now. Some of them will end up with imaging they didn't need, surgical referrals that weren't warranted, and operations that won't help them.
A physician-led MSK model doesn't mean more specialist visits or higher unit costs. It means better triage from the start, so every patient gets exactly the level of care their condition requires, no more and no less.
For employers and health plans, the impact is straightforward:
- Fewer unnecessary MRIs
- Fewer inappropriate surgical referrals
- Lower total cost of care
- and employees who get better faster, and stay better.
The cascade is predictable. So is the solution.
MSK cost is a decision problem. And the right decision, made at the right time by the right clinical team, changes everything downstream. That's what Vori was built to do.
About Vori Health
Vori Health is a physician-led MSK medical practice — a fundamentally different model from traditional MSK programs. By putting clinical expertise at the front of the care journey, Vori ensures every patient gets exactly the care their condition requires: no more, no less. The result is fewer unnecessary procedures, lower total cost of care, and better outcomes for member, organizations and plans alike.
Clinical data referenced in this post is sourced from Dr. Mary O'Connor's clinical review (April 2026), Vori internal outcomes data, and published peer-reviewed literature. Citations available upon request.
Learn more at vorihealth.com.
.png)

